

Table of Contents
Affiliate link notice: As an affiliate of BetterHelp and other third-party vendors, we may receive compensation if you make a purchase using the links provided on this page. For more information, visit our disclosure page.
Last Updated on March 29, 2026 by Randy Withers
Most people think healthcare access in rural America is a distance problem.
They picture long drives, fewer hospitals, and limited specialist care. And while those barriers are real, they only scratch the surface. What often gets missed is what happens after access breaks down—when care is delayed, inconsistent, or simply unavailable. That’s where the problem shifts from logistical to clinical, and increasingly, psychological.
Living in rural communities still offers what it always has: space, quiet, and strong social ties. But those advantages exist alongside a growing reality—many rural residents are navigating serious health concerns, including mental health conditions, with fewer resources, fewer providers, and fewer opportunities for early intervention. Over time, that gap doesn’t just inconvenience people. It compounds risk.
Healthcare systems in these areas are under strain. Workforce shortages, geographic isolation, and an aging population all contribute to a fragile infrastructure that struggles to meet demand. Nurses and advanced practice providers have stepped in to help bridge that gap, particularly those who have completed a psych NP program, offering both medical and mental health support in communities that often lack both.
This article takes a closer look at why healthcare access in rural America is not just a matter of proximity—it is a mental health issue with far-reaching consequences. The factors driving this crisis are not isolated; they are layered, reinforcing, and, in many cases, worsening. Understanding them is the first step toward addressing a problem that affects not just where people live, but how well they live.

Why This Matters More Than You Think
It is easy to frame healthcare access in rural America as an inconvenience. Longer drives. Fewer providers. Limited appointment availability. But those descriptions minimize what is actually happening on the ground.
When access is limited, care is delayed. When care is delayed, conditions worsen. And when conditions worsen—especially mental health conditions—the outcomes become harder to reverse.
Rural populations already face elevated risks across several domains. Chronic illness rates are higher. Preventive care is less consistent. Mental health services are often scarce or entirely absent. These are not isolated issues; they interact. A patient managing diabetes without consistent follow-up may also be dealing with untreated depression. A person struggling with substance use may have no realistic access to ongoing counseling or medication management. Over time, the system does not just fail to intervene—it allows problems to compound.
The data supports this reality. According to the Rural Health Information Hub, a significant proportion of designated shortage areas are located in rural regions, where provider availability simply cannot meet demand. In practical terms, that means fewer entry points into care and fewer opportunities to stabilize conditions early.
This is where the conversation shifts. Limited access is not just about inconvenience or geography. It directly affects disease progression, treatment adherence, and overall quality of life. In mental health, where consistency and continuity are essential, even small disruptions can have outsized consequences.
The sections that follow outline how these barriers operate in real terms—and why they are better understood as components of a broader mental health crisis rather than a simple access issue.
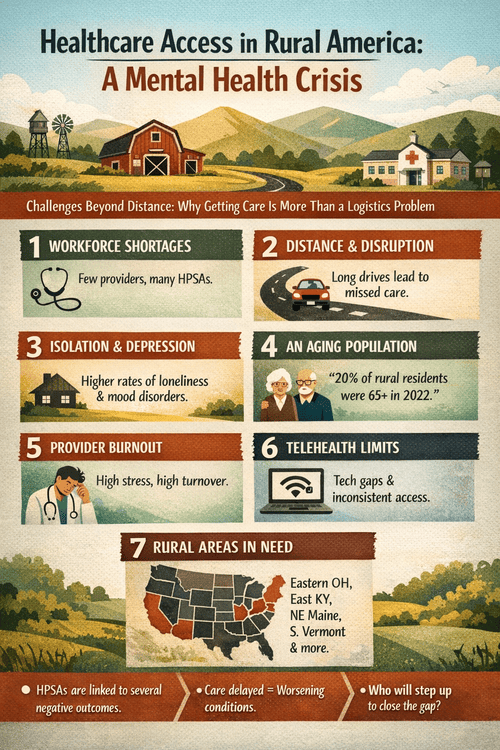
1. Workforce Shortages Are Creating Mental Health Deserts
The most immediate and measurable driver of healthcare access issues in rural America is the workforce shortage. This is not a subtle gap—it is a structural deficit that affects nearly every level of care.
A disproportionate number of Health Professional Shortage Areas (HPSAs) are located in rural communities, where the supply of providers cannot meet even basic demand. In practical terms, this means fewer primary care physicians, fewer specialists, and critically, far fewer mental health providers.
The consequences are not abstract. In many rural areas, patients face wait times that stretch weeks or months. Some communities have no practicing psychiatrist at all. Therapy services, if available, may be limited to brief, inconsistent care or require significant travel. For individuals dealing with depression, anxiety, trauma, or substance use, that delay is not neutral—it allows symptoms to intensify.
HPSAs are linked to several negative outcomes, including:
- higher rates of chronic illness
- increased provider burnout
- worse self-reported health status
- reduced access to timely care
These outcomes reinforce each other. As providers become overextended, burnout increases. As burnout increases, turnover follows. And as providers leave, access shrinks even further.
From a clinical standpoint, this creates what can reasonably be described as mental health deserts—regions where the need for care exists, but the infrastructure to deliver it does not.
For those entering the field, particularly advanced practice clinicians, this gap is not just a problem—it is a point of entry. Psychiatric nurse practitioners, in particular, are uniquely positioned to address these shortages. With training that spans both medical and mental health domains, they can provide assessment, diagnosis, and treatment in settings where no other specialized care exists.
The shortage is not temporary, and it is not resolving on its own. It is reshaping how and where care is delivered—and who steps in to provide it.
2. Distance Isn’t Just Inconvenient—It Disrupts Continuity of Care
Distance is often described as the defining challenge of healthcare access in rural America, but the issue is not simply the miles between a patient and a provider. It is what those miles do to consistency.
Care that requires long travel is care that is easier to delay, reschedule, or abandon altogether. A routine follow-up becomes a half-day commitment. A therapy session requires time off work, childcare coordination, and transportation planning. Over time, even motivated patients begin to miss appointments—not out of neglect, but because the logistics become unsustainable.
A patient managing depression may start strong—attending sessions regularly, beginning medication, making incremental progress. But when each appointment requires a 45-minute drive each way, missed work, and coordination at home, the pattern often breaks. One missed session becomes two. Medication follow-up gets delayed. Symptoms return—not suddenly, but predictably.
From a clinical standpoint, this matters more than access alone. Continuity of care is what stabilizes chronic conditions and supports mental health treatment. When that continuity breaks down, outcomes shift. Medications are taken inconsistently. Therapy loses momentum. Early warning signs go unaddressed.
In mental health specifically, gaps in care can carry disproportionate risk. A missed session is not just a missed conversation—it can mean the difference between stabilization and escalation. In rural settings, where alternative providers are often unavailable, those gaps are harder to recover from.
Distance, then, is not just a barrier to entry. It is a barrier to staying engaged in care—and that distinction is where the real impact shows up.
3. Rural Populations Experience Higher Rates of Isolation and Depression
One of the less visible aspects of healthcare access in rural America is social isolation. While rural communities are often described as close-knit, that reality is not universal—and even when it is, geographic spread and limited resources can still create meaningful isolation.
Fewer social outlets, fewer behavioral health services, and fewer opportunities for connection all contribute to a quieter but significant risk factor: prolonged loneliness. Over time, isolation becomes more than a social issue. It becomes a clinical one.
Depression, anxiety, and substance use disorders tend to thrive in environments where support is limited and stigma remains high. In many rural areas, seeking mental health care still carries a degree of visibility that deters people from pursuing it. When the nearest provider is also a familiar face in the community, privacy concerns become another barrier layered onto access.
The result is a pattern clinicians recognize quickly: symptoms go unaddressed until they intensify. By the time care is sought, conditions are often more severe and more complex.
This is where the distinction between access and outcome becomes clear. It is not simply that services are harder to reach. It is that the absence of those services allows mental health conditions to deepen in ways that are harder to reverse.
4. The Aging Population Is Increasing Mental Health Complexity
The United States population is aging, which is happening more rapidly in rural areas than in urban areas. In 2022, 20% of rural residents were ages 65 or older, up from 15% in 2000.
This shift carries significant clinical implications. Older adults are more likely to experience chronic medical conditions, cognitive decline, and complex medication needs. They are also at increased risk for depression, particularly when combined with factors like isolation, loss of independence, and limited access to care.
In rural settings, these challenges are magnified. Geriatric specialists are scarce. Mental health services for older adults are even more limited. Care often falls to overextended primary providers or family members who may not have the training or resources to manage complex conditions effectively.
At the same time, the aging population is contributing to the workforce shortage itself. Many experienced healthcare professionals are nearing retirement, reducing the supply of providers just as demand is increasing.
This creates a compounding effect: more patients with complex needs, fewer providers to treat them, and a system that becomes progressively harder to navigate.
In mental health care, where time, consistency, and specialization matter, that strain is felt quickly—and often most acutely by those who are least equipped to adapt to it.
5. Burnout and Provider Turnover Are Making a Fragile System Worse
Even when providers are present, the system remains unstable. Workforce shortages do not just reduce access—they increase pressure on the clinicians who remain.
In rural settings, providers often carry broader caseloads with fewer resources. A primary care provider may also be managing behavioral health concerns. A nurse practitioner may be functioning with a level of autonomy that would typically be distributed across a larger team. Over time, that strain accumulates.
Burnout in these environments is not surprising. It is predictable.
As burnout increases, so does turnover. And turnover has consequences that extend beyond staffing numbers. Patients lose continuity. Trust is disrupted. Treatment plans stall or reset entirely. In mental health care, where rapport and consistency are central to progress, that disruption can be particularly damaging.
This creates a feedback loop. Fewer providers lead to more strain. More strain leads to more burnout. More burnout leads to more providers leaving. Each cycle tightens the bottleneck.
From a systems perspective, the issue is not just recruitment—it is retention. Without stability in the workforce, even well-intentioned efforts to expand access struggle to take hold.
6. Telehealth Helps—but It Doesn’t Fully Close the Gap
Telehealth is often presented as the solution to healthcare access in rural America, and in many cases, it does meaningfully improve access. It reduces travel time. It allows for more frequent follow-ups. It expands the reach of specialists into underserved areas.
But it is not a complete solution.
Access to reliable broadband remains inconsistent in many rural regions. Technology literacy varies, particularly among older populations. And certain types of care—especially those involving complex assessments or severe mental health conditions—do not translate seamlessly to a virtual format.
There are also limitations that are less obvious. Privacy can be difficult to maintain in small or shared living environments. Engagement may be lower when care is delivered through a screen. And for some patients, the therapeutic connection is simply harder to establish without in-person interaction.
This does not diminish the value of telehealth. It remains an important tool. But it is best understood as a partial solution layered onto a larger problem—not a replacement for a fully functioning healthcare system.
7. Rural Healthcare Creates Immediate Impact for Clinicians Willing to Step In
The same factors that make healthcare access in rural America so challenging also create a unique opportunity for clinicians entering the field.
In high-resource environments, roles are often specialized and narrowly defined. In rural settings, the opposite is true. Providers are needed to do more, learn faster, and adapt to a wider range of clinical situations.
This is particularly true for those pursuing advanced practice roles in mental health. Psychiatric nurse practitioners are positioned to address multiple gaps at once—assessment, diagnosis, medication management, and, in some cases, therapeutic support. In areas where mental health services are limited or nonexistent, that scope becomes immediately impactful.
Below is a list of a few rural areas that require more healthcare professionals, according to Nursing Education and the US Bureau of Labor Statistics.
- Eastern Ohio
- East Kentucky
- Northeast Maine
- Southern Vermont
- South Nebraska
- Southeast Missouri
- Southwest Maine
- Southwest Iowa
These are not just locations with job openings. They are communities where access to care is limited and where additional providers can meaningfully change outcomes.
What This Means for Future Psychiatric Nurse Practitioners
For those considering a career in mental health, the realities of healthcare access in rural America are not just a problem to understand—they represent a gap in care that clinicians are actively being called to fill.
The need is not abstract. In many rural communities, there is no consistent access to psychiatric care. Primary care providers often carry the burden of managing mental health conditions without specialized training, and patients may go months—or longer—without appropriate diagnosis or treatment. That kind of gap creates space for clinicians who can operate with both autonomy and breadth.
Psychiatric nurse practitioners are uniquely positioned in this landscape. Their training allows them to assess, diagnose, prescribe, and manage care across a range of conditions, often serving as the primary mental health provider in underserved areas. In settings where the system is stretched thin, that level of versatility becomes essential rather than optional.
There is also a professional reality worth acknowledging. Rural practice environments often provide greater clinical responsibility, faster skill development, a broader scope of practice, and, in many cases, stronger job stability.
But the appeal should not be reduced to opportunity alone. The work carries weight. Patients may present later in the course of illness. Resources may be limited. Progress can be slower and less linear. It requires a level of adaptability and resilience that is not always emphasized in training.
For those willing to engage with that reality, however, the impact is immediate and visible. In rural settings, access is not an abstract concept—it is something clinicians either provide or patients go without.
Final Thoughts
Healthcare access in rural America is often described in terms of distance, provider shortages, and infrastructure gaps. Those factors matter. But they do not fully capture what is happening.
At its core, this is a mental health issue.
When care is difficult to access, people wait. When they wait, conditions worsen. When conditions worsen—particularly in mental health—the path back becomes more complicated, more resource-intensive, and less predictable. Over time, the system does not just fail to meet demand. It allows problems to deepen.
The factors outlined here—workforce shortages, geographic barriers, isolation, aging populations, provider burnout, and partial solutions like telehealth—do not operate independently. They reinforce each other. Each one adds pressure to a system that is already strained, and the result is a pattern of care that is inconsistent, delayed, or unavailable when it is most needed.
But there is another side to this.
The same gaps that define healthcare access in rural America also define where meaningful change is possible. For clinicians, particularly those entering mental health fields, these environments offer a level of impact that is difficult to replicate elsewhere. The work is not easier. It is often more demanding. But it is also more direct.
This is not simply a question of where care is delivered. It is a question of whether it is delivered at all.
In rural America, access to care is not assumed. It is negotiated—and often lost.
And in many communities, what happens next still depends on who is willing to show up.






Great article! This topic deserves more attention because mental health access in rural areas is still a major challenge for many people.